5 risk factor for hypertension1) Hypertension
2) Cigarette smoking
3) Physical inactivity
4) Diabetes Mellitus
5) Dyslipidaemia
5 fundoscopic changes in severe hypertension1) Hemorrhages
2) Exudates
3) Papilloedema
4) Arteriolar narrowing
5) Swollen optic nerve
5 causes of secondary hypertension1) Sleep apnoea
2) Acromegaly
3) Coarctation of aorta
4) Chronic kidney disease
5) Thyroid or parathyroid disease
5 classes of antihypertensive medication1) ACE inhibitors
2) Angiotensin Receptor Blockers
3) Beta-blockers
4) Calcium Channel Blockers
5) Diuretics
5 features of malignant hypertension1) Numbness of the arms, legs, face or other areas
2) Changes in mental status – confusion, decreased alertness
3) Seizure
4) Shortness of breath
5) Blurred vision
5 investigations in primary hypertension with reason1) ECG – left ventricular hypertrophy ( target organ damage)
2) Fasting blood sugar – diabetes (risk factor)
3) Renal function test – chronic kidney disease ( target organ damage)
4) Lipid profile – Dyslipidaemia (risk factor)
5) Chest X ray – heart failure ( target organ damage)
List 2 medication that is preferred in1) Hypertension + diabetes – ACEi & ARB
2) Hypertension + ischemic heart disease – ACEi & Beta-blockers
3) Hypertension + congestive heart failure – diuretic & ACEi
4) Hypertension + chronic renal failure – ACEi & ARB
5) Hypertension + hypertensive crisis – CCB & Beta-blockers
5 complications of hypertension1) Left ventricular hypertrophy
2) Angina or myocardial infarction
3) Heart failure
4) Chronic kidney disease
5) Stroke/ transient ischemic attack
5 pathophysiological changes that increase blood pressure5 advices to patient with hypertension on discharge1) If you are overweight, try to lose weight
2) Reduce salt intake
3) Exercise regularly
4) Moderate alcohol intake
5) Stop smoking
5 common side effect of hypertension and which class it associated with1) Diuretics – hypokalemia
2) Beta-blockers – erectile dysfunction
3) Calcium channel blocker – ankle oedema
4) ACEi - cough
5) Alpha-1-adrenergic blockers – postural hypotension
5 drugs to prevent recurrent stroke1) ACEi
2) Diuretic
3) ARB
4) Warfarin
5) Aspirin
5 different types of cerebrovascular accident1) Subarachnoid hemorrhage
2) Subdural hemorrhage
3) Intraparenchymal hemorrhage
4) Epidural hemorrhage
5) Ischemic stroke
5 signs of overdose antihypertensive1) Bradycardia
2) Hypotension
3) Altered mental status
4) Seizures
5) Angioedema (ACEi)

- sudden traction
- radial head sublaxation

- tibial tubercle apophyseal traction injury
- rupture of the growth plate at the tibial tuberosity
- tibial tubercle hurt
- caused by overuse

- popliteal cyst
- non-pulsatile swelling
- posterior aspect of the knee
- Ddx - lipoma, aneurysm, neuroma & rarely tumor


- physical examination - Adams test (forward bending)

- Slipped capital femoral epiphysis (also known as "Slipped upper femoral epiphysis")
- referring to a fracture through the physis (the growth plate), which results in slippage of the overlying epiphysis
- a/w obesity, deficient gonadal development & hypothyroidism

- developmental dysplasia of the hip
- patients who are born with dislocation or instability of the hip, which may then result in hip dysplasia


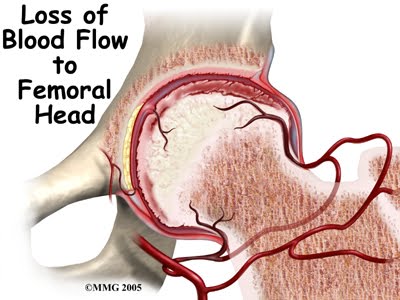
- avascular necrosis of femoral head
- X-ray - wide articular surface, then necrosis - flattened femoral head - later becomes spherical

- swelling of the scalp
- involves presenting part
- caused by the pressure exerted on the part during labor and delivery
- involving the scalp only
- crosses suture lines
- resolves quickly over several days


- subperiosteal bleed
- limited to bone
- does not cross suture line
- a/w overlying non-depressed skull fracture
- slow bleeders - not present at birth
- increase in size in few days
- a rim can be felt around the edge
- resolve spontaneously over several months
- can be fooled by bilateral cephalhematomas
- common cause of jaundice

- tan or light brown lesions
- can occur anywhere
- vary in size
- sharply demarcated

- seen in infancy
- yellow-orange plaques resembling flat warts
- located on scalp
- have potential to become malignant
- usually removed

- macular lesions
- quickly grow in the 1st year of life
- occur anywhere
- bright red, reminiscent of a strawberry
- tx not necessary
- regress spontaneously
- + stridor - subglottic hemangioma

- seen over the eyelids, glabella, nuchal area
- flat vascular lesion
- disappear with time
- DDx - Port wine stains (permanent & unilateral)
- becomes darker red when cries

- response to circulating androgenic hormones
- rarely require therapy

- vasomotor response to cold stress
- lacy pattern - cobblestone
- seen in trisomy 21, trisomy 18

- small inclusion cyst and are pearly white
- in mouth - known as Epstein's pearls


- small papules / pustules
- NOT in 1st day of life
- if scraped - fulls with eosinophil
- DDx: SSSS (stapylococcal scalded skin syndrome)
- How to differentiate? SSSS - if scraped, full with neutrophil, infant looks very ill, Nikolsky sign (gentle stroking of the skin causes the skin to separate at the epidermis)

- Usually at presacral area
- Ddx: bruise
- How to differentiate? Bruise - fade into surrounding skin, Mongolian spot - obvious different colour